| Structure | Name/CAS No. | Articles |
|---|---|---|
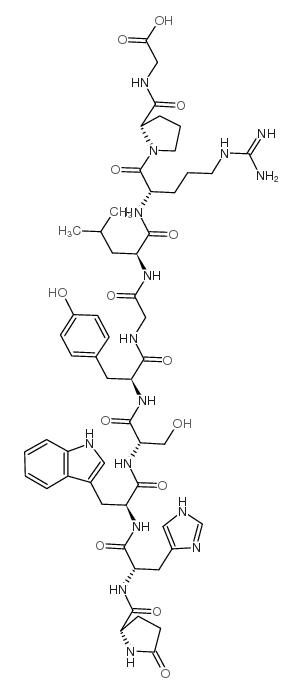 |
LHRH (free acid) trifluoroacetate salt
CAS:35263-73-1 |
|
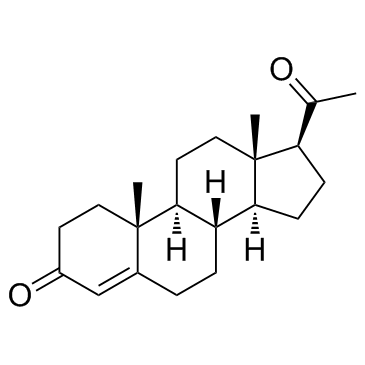 |
Progesterone
CAS:57-83-0 |
|
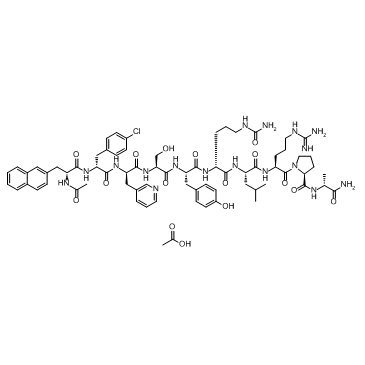 |
Cetrorelix Acetate
CAS:145672-81-7 |
|
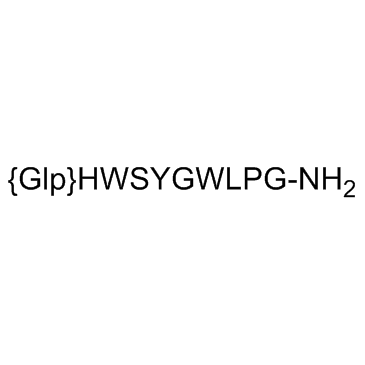 |
LHRH (salmon) acetate salt
CAS:86073-88-3 |