| Structure | Name/CAS No. | Articles |
|---|---|---|
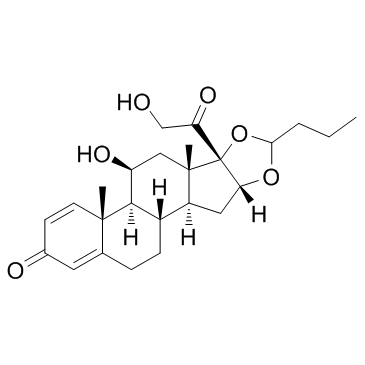 |
Budesonide
CAS:51333-22-3 |
|
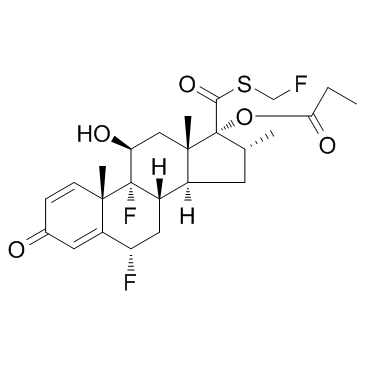 |
Fluticasone propionate
CAS:80474-14-2 |
|
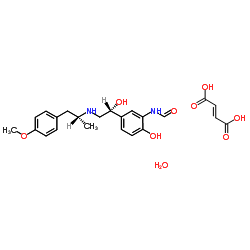 |
formoterol fumarate dihydrate
CAS:183814-30-4 |