| 结构式 | 名称/CAS号 | 全部文献 |
|---|---|---|
 |
阿司匹林
CAS:50-78-2 |
|
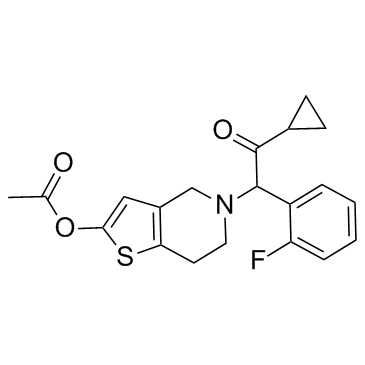 |
普拉格雷
CAS:150322-43-3 |
|
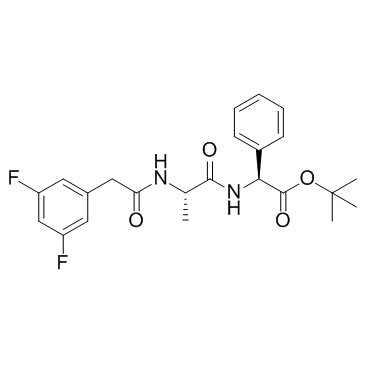 |
DAPT (GSI-IX)
CAS:208255-80-5 |